

Is your child now ready for more autonomy? What is too much, too soon? How to coach, manage risk, experiment, and deal with uncertainty. We explore school, exercise, holidays, rule-free eating, body image, preparation for college, relapse prevention, and total recovery.
Extracts from Chapter 10 of 'Anorexia and other eating disorders – how to help your child eat well and be well'
This chapter really matters as this phase of the treatment is often overlooked, or so poorly managed that youngsters decline and all the earlier hard work is lost.
If you're tired of reading, this phase is also covered in my Bitesize audio collection.

Steps to independence and total recovery
So far we’ve taken responsibility for meals and behaviours. That’s the first phase of treatment, where we focus on restoring health and weight. We’ve also done exposure work (Chapter 9) to address fears and bring back ‘normal’ behaviours. Now comes the work of guiding our kids back to an age-appropriate level of independence. It’s like teaching a child to ride a bike without training wheels — we run alongside to keep them steady until they can balance on their own. Or when a cast comes off a broken leg – rehab is needed before they can skip, and run freely again.
In Family-Based Treatment (FBT) the transition from parental decision-making to independence is called ‘Phase 2’. More precisely: “responsibility over eating is gradually handed back to the adolescent to whatever extent is age-appropriate and typical for that particular family.” There’s also a ‘Phase 3’, which “involves a review of healthy adolescence and an assessment of where the adolescent is developmentally once the ED has receded” and aspects of this are dotted about this book.
When does ‘Phase 2’ begin?
Paraphrasing the FBT manual, you begin Phase 2 when your child isn’t fighting meals or weight gain any more. But instead of rigid ‘phases,’ I find it helpful to work with the little pockets of independence a person is almost ready for. Today your son may be able to choose his snack, and next week he may manage it in school with minimal supervision. But it could be too early for a return to the gym. Is he ready for a sleepover? Great! But you won’t yet let him go on a week-long school trip.
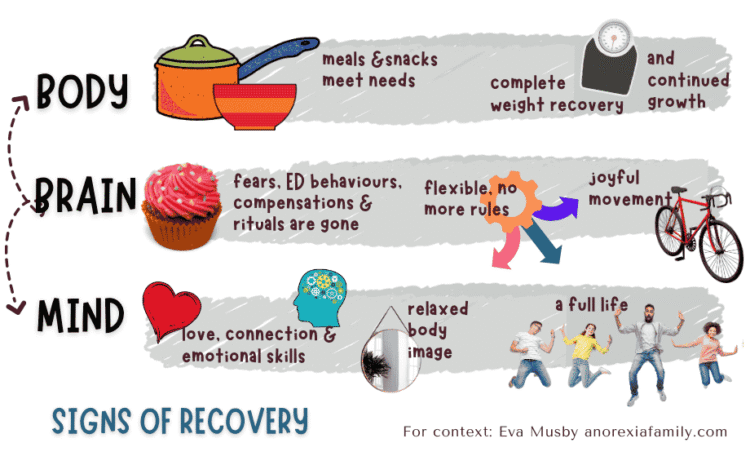
Here’s my graphic once more to show how the tasks of recovery fit together:

It's not a cliff edge
The FBT manual doesn’t ask families to jump off a cliff. We are to “maintain parental management of eating disorder symptoms until the patient shows evidence that she is able to eat well and gain weight independently”. We’re to go back a step if independence isn’t working: “If the patient returns to dieting or loses weight, therapists should swiftly motivate parents to re-establish control over eating”. A young person should know that when they’re given some autonomy, it’s an experiment. That their parents will step in if it’s not working, or if they go through a significant setback.

A risk management framework
How can we know that our children are ready for a piece of autonomy? We don’t. Their true thoughts are hidden from us, and the more independence we give them, the less we’re able to observe. So how do we handle the uncertainty? We could forever micromanage our children, but then they’d make no progress. Or we could just hope for the best as we hand over independence. Neither is great. Instead, I propose a risk management approach.
Let’s start with a metaphor. We long for our children to fly with their own wings. If they don’t yet have the capability for it, they’ll crash. So, we work on strengthening those wings (as in the previous chapters). We set up flying practice. We do trial runs over soft ground. Only then do we let our fledglings fly freely. And for quite a while, our role isn’t over. We continue to watch how they navigate unusual situations – illnesses, gusts of change. We stay ready to intervene if required.
Armed with a risk-management framework, we can be brave and make fast progress despite uncertainties – and that’s because nothing too bad can happen. Here’s a flowchart to offer you some structure.
[Jumping to another section of the chapter…]
Healing your child's mindset
You’re aiming for full recovery, and it’s helpful for your child to see your confidence that she’ll get there. Friends and therapists may already believe she’s doing great. But you know how much she still needs you to keep her afloat. Perhaps she’s burdened by anxieties about body shape, disquiet about sensations in her belly after a big meal, a surge of alarm when a waiter brings an oily dish, some nervousness when an illness requires bed rest. Perhaps there are psychological issues, whether or not they pre-dated the eating disorder: feeling worthless and unlovable, the compulsion to do everything to perfection, an anxious nature, or trauma.
The good news is that your child can behave wisely even when thoughts of restriction pop up. This discipline can help her function safely for the long term.
But you’re more ambitious. You want her mind to be free from eating disorder thoughts and anxieties. This might be a good time for some individual psychotherapy (more in Chapter 12), group therapy, or the body-image component of Cognitive Behavioural Therapy for eating disorders.
Could one of these therapies be the final piece in shifting your child’s mindset? Maybe yes, and maybe no. At the very least, it should give her tools to manage whatever her mind is throwing at her. If psychotherapy is on your radar, go for it. Be aware, though, that often our children do not engage: in this case it’s a pointless and miserable exercise. I’d also turn down a therapist who is so focused on autonomy that you get stripped of your power ever to support your child again.
[Jumping to another section of the chapter…]
Is your child getting discharged from treatment too early?
Sadly, a frequent issue is that youngsters are discharged well before recovery. To help you to advocate for your child, take a look at my graphic showing signs of recovery.
When discharge feels rushed, often there’s not been much work on extinguishing fears (Chapter 9) or on independence (Phase 2). You could get the impression that treatment is merely about refeeding and reaching some arbitrary weight percentile.
Some clinicians discharge as soon as a person is relatively stable because – as we’ll see later – they don’t believe that full recovery is possible.
Another reason for early discharge is the pressure clinicians face from huge waiting lists. Ideally, they’d express their regret and empower parents to continue the work without them. The problem is when they cheerlead: ‘You’re doing so well! You’re going to be fine! Relax, mum and dad!’ This disempowers parents – indeed, it fails to inform them that there’s more to do. Meanwhile, the young person, who’s still suffering, feels hopeless and believes they’re a failure. They might think they’re ‘not sick enough’ or unworthy of further help.
Sadly there are clinicians who, rather than recognising that treatment failed the child, blame the child for not engaging with treatment and not opening up to a particular therapist. Let’s be clear: if treatment isn’t working, professionals should be guiding you to alternatives (see Chapter 12) – not discharging.
You may not have the power – or the funds – to keep your child in treatment. Even if you do, you might sense that your clinicians have reached the limits of their expertise. If formal treatment ends early, with or without your agreement, here’s something that may help. Get the professionals to validate a plan for the work to continue at home – it’s a message your child needs to hear. You could base your plan on the flowcharts in this chapter and Chapter 9. Careful! This is different from a ‘relapse prevention’ plan. Relapse prevention is for after your child has fully recovered, not while there’s still so much work to do.
[Jumping to another section of the chapter…]
Progressing through school
In Chapter 6 I described flexible levels of support at school, particularly around meals. Another layer you may need to navigate is the school's approach to weight bias, ‘healthy eating’ and exercise. Many clinicians and parents will tell you that health promotion messages are a top precipitating factor for a child’s eating disorder
How can you protect your child from further harmful messages? And can you help them build resilience for body-shaming culture general?
‘Health promotion’ in school
At school, my daughter was made to keep a food diary, read nutritional labels, and count dietary fat units. She was told that sweets were bad, yet they were handed out as rewards for good work. She got to watch a ‘gross’ liposuction video. And when ‘friends’ thought it was OK to fat-tease on the playground, she decided she’d be thinner than all of them. I bet you have your own horror stories.
Teachers are required to deliver ‘health promotion’ without any training. So they perpetuate society’s madness. Food is labelled as ‘healthy’ or ‘junk’, ‘good’ or ‘bad’. You can never eat lean enough, you can never exercise too much. Thinness is holy, while a large body suggests sloth and terrible health. Governments require schools to weigh children, who internalise that a low number is best. Parents receive letters informing them their child is ‘obese’ and should lose weight, based only on a statistical BMI calculation.
What are your options?
[Jumping to another section of the chapter…]
Food and freedom after weight recovery
Once your child is (probably) weight-recovered, you’ll be wondering how much to feed and how much independence to give them. Their needs and abilities will be specific to them and will evolve with time. I hope the following suggestions help you in your experiments and your discussions with professionals.
[Jumping to another section of the chapter…]
Rule-based or intuitive eating?
Trusting my body’s eating cues has worked for me pleasantly all my adult life. When it comes to food, I’m not interested in rules, willpower or self-discipline. So I was glad to find resources on ‘intuitive eating’ by Tribole and Resch.
Think of appetite and fullness like your phone’s battery indicator. When it’s accurate, you know when to recharge — that’s intuitive eating. When it’s not, your body still needs energy, so you need another method to guide how much and when to eat.
Does complete recovery for your child mean that they’ll eat intuitively, or will they need to keep a system – some level of rule-based or structured eating? Answers are likely to be individual. Not everyone has the biological or mental makeup for intuitive eating. Some people with ARFID never get hungry. And some people find it hard to feel satiated. For a while, your child may experience eating as a complicated, non-intuitive business. Remember that the biology of appetite regulation is complex and can take a while to settle after the metabolic disruptions your child has been through. If their appetite cues were reliable before the eating disorder, hopefully they’ll return. If not, intuitive eating is not for them.
At first, your child may benefit from some rules – you could call it ‘structure’ or ‘scaffolding’ – for balanced, regular, sufficient eating and exercise. Gradually, you’ll see which rules can safely be reduced or discarded. Rules may morph into rough guidelines, and in some years, your child may find that their intuition is a reliable friend again. Don’t rush it. Treat it like a series of small, low-risk experiments. If something goes wrong, go back to what worked and get some stability before trying again.
Your child’s best tool is to know themselves. Does their body give them reliable cues? How do emotions or stress affect them? Can they eat intuitively most of the time, but lose their appetite when upset? Perhaps they need a rule to ‘Eat even when I’m distressed.’ Rules are compatible with complete recovery if they’re not too intrusive and genuinely aligned with health and wellbeing.
[Jumping to another section of the chapter…]
Body image may still be poor
For body image to return to ‘normal’, weight recovery is essential:
“I realized that in energy balance, I was freer to think about much more meaningful and interesting things in life than food, weight, and exercise”
As always, weight restoration is necessary but not sufficient. And while work on exposure and independence tends to improve body image, it rarely provides a complete fix. In a world steeped in fat-shaming pressures, the task is considerable! It’s a credit to our teens that they can eat independently and wisely, even while continuing to see themselves as fat (or not muscular enough).
Body image transformation needs time. Perhaps that’s because time creates opportunities for a rich, interesting life. It also gives us, as parents, the chance to model a positive attitude and to have conversations that nurture reflection and self-kindness. See my suggestions in Chapter 14 in the ‘Am I fat?’ section.
[Jumping to another section of the chapter…]
Safeguards as your child leaves the nest
Is your child ready to leave home?
The usual advice is for a young person to have at least six symptom-free months before they leave home. We can’t be sure what goes on in their heads, but if all the behaviours are good, chances are that as their life expands, their recovery will strengthen.
Without six clear months of symptom-free stability, we risk having to bring our children home by Christmas—costing them the rest of the academic year. I also know of many young people who have been limping through university, unable to fully engage: they can’t eat socially, are beholden to an exercise program, and get overwhelmed by exams. The parents, without a clear picture, either give up or try to monitor and guide from a distance. Some make frequent visits or rent a place near the university. It’s an unpleasant time for all.
So pay attention to your gut. I speak to parents whose child successfully delayed university for a year, perhaps attending a short course in a local institution or enjoying a part-time job.
[End of extract from the chapter]
In this chapter:
- Steps to independence and total recovery
- When does 'Phase 2' begin?
- It's not a cliff edge
- A risk management framework
- Supervising and monitoring
- Healing your child's mindset
- Individualise the pace to your child
- Collaboration
- Independence will take the time it takes
- Our story: both freedom and vigilance
- Our story: letting time (and some collaboration) do the last bits
- Watch out for these issues
- Is your child getting discharged from treatment too early?
- Is the push for independence too soon, too fast?
- Is your child now resisting your support?
- Weight recovery is not the same as recovery from an eating disorder
- Parents deal with uncertainty — it's not codependency
- Progressing through school
- 'Health promotion' in schools: why, oh why?
- Risk-reduction programs in schools
- Re-introducing exercise
- Activities
- Holidays and school trips: risky or beneficial?
- Food and freedom ater weight recovery
- Should you reduce quantities?
- What's your child believing?
- We parents evolve as well
- Rule-based or intuitive eating?
- What if your child eats 'too much'?
- When to ditch the scales?
- Addressing depression, OCD and other anxiety disorders
- Trauma, grief and re-engaging with life to the full
- Normal teenage behaviour or eating disorder?
- Body image may still be poor
- Dealing with relapse
- Events that rock the boat
- Flu and stomach bugs
- Relapse prevention, plans and contracts
- Prepare your child to leave home
- Safeguards as your child leaves the nest
- Is your child ready to leave home?
- Safeguards if your child is not yet recovered
- Safeguards if your child is well
- Is there such a thing as total recovery?
- Will parents always have to worry?
Where to next?
* See also: Guidance for schools *
* See also: School trip or Summer camp flowchart *
* See also: Phase 2 – How to guide your child to complete recovery from an eating disorder *
* See also: Weight-restoration: why and how much weight gain? *
* See also: How to overcome weight bias and fat phobia *
* Next: Chapter 11: Parents, friends, family and work: help or hindrance? *
Leave a Reply