Your cart is currently empty!


What do BMI and Weight-For-Height mean?
#Links: weight-target
Clinicians often talk in terms of Body Mass Index (BMI). For children and teenagers, some use Weight-For-Height. Some use 'BMI z score'. In this post I'll explain what these measures are and how they are usually misused.
If you prefer watching a 10mn video, it says most of what's on this page:
What's BMI or Weight-for-height got to do with your child's health?
Hardly anything, is the answer. Unless it's terribly low (but then just eyeballing your child and noting symptoms would tell you that).
Here's the problem. A child can wrongly be declared healthy (or not), based on their BMI or Weight-for-height. Particularly worrying is the trend for schools to send letters to parents, warning them that their child should lose weight, based on BMI.
Another common situation, if your child has anorexia or another eating disorder which caused them weight loss, is for a therapist to set your child's target weight based on body-mass index (BMI) or weight-for-height (FWH). In another post I explain the problem with that.
If you're wondering what BMI means, or '95 percent'weight-for-height' and, why there's a problem with the way these are used, read on.
What is body-mass index (BMI)?
It's the person's weight (in kilos) divided by the square of their height (in metres). For a given height, the bigger the BMI, the heavier you are.
Statisticians have done big population surveys of people's BMIs and produced tables and charts. They have labelled various BMI ranges as 'healthy', 'underweight', 'overweight', and so on.
Statistically, populations in the 'underweight' and 'overweight' BMI ranges are associated with poorer health, but like most things statistical, that doesn't say much about any individual (besides, there's huge controversy around those BMI categories and their relationship to health). You can't tell if a person is (or will be) healthy or ill based on a BMI number.
"Health is not a number on weight scales"
Simon Chapman, Paediatrician, Child and Adolescent Eating Disorders Service, South London and Maudsley NHS Foundation Trust
Unless their BMI is particularly high or low, you can't even tell if a person will look large or thin. I mention this because in our society, there's anxiety around 'looks'. BMI doesn't account for muscle or fat ratios, bone structure, heredity, the body shape that nature intended for you, what your body needs right now, and so on.
BMI charts represent the range that exists among humans, not what any particular person should be. Yet everywhere — at doctors' surgeries, on health websites — there are prompts to use BMI charts as a source of advice. You have probably seen charts like this one for male or female adults:
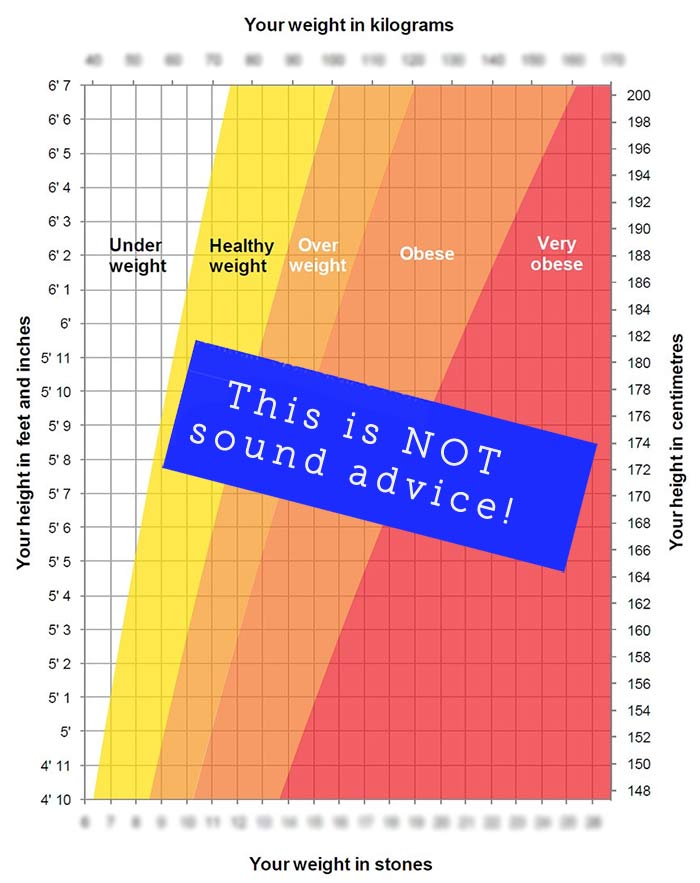
The "Your weight", "Your height" on the chart, implies personal advice. To not be part of the problem, I've obscured the numbers. Before I knew anything about eating disorders, when I saw charts like this I'd wonder, 'Am I weird? How could this apply to me?'. I would be an impossible shadow of myself at one end of the supposedly 'healthy' range, and at the other end, I'd have to find special clothes shops.
Notice that this chart has lumped together adults of any age, both male and female. Young adult? Past the menopause? Elderly? It's all the same on this chart, whereas in truth bodies keep changing and having different needs.
For children, most experts recognise BMI varies a lot during childhood, and between boys and girls, so as we'll see further, the data is presented differently.
Using BMI to say anything about an individual is like using a chart to predict what size shoe you need. If I had a shoe shop I might amuse myself by labelling the smaller shoes 'Dwarfs' and the bigger ones 'Giants'. In the middle, I could have 'Normals'. I could even label the exact middle size 'Ideal'. None of this would make any difference to the size of shoe my next customer needs. But it would cause a lot of confusion.

Some of the BMI charts or calculators warn you against using the data as advice (while still displaying the data as if it were advice):
From a health organisation US calculator:
"Please keep in mind that this BMI calculator is not meant to serve as a source of clinical guidance […] Persons may consider seeking advice from their healthcare providers on healthy weight status."
The UK's health service calculator just says:
"If you have an eating disorder, the BMI calculator results don't apply."
Before I explain how BMI, and how 'Weight-for-height', is used in children, let me take the mystery out of 'percentiles'.
What does 'percentile' mean?
Here's the meaning of 'percentile' or 'centile'.
Line up 100 girls of the same age in order of height. The 75th along is among the tallest, at 75 percentile height. The one in the middle has median height: 50th percentile.

You could line the girls up in order of weight, or in order of body-mass index, and get percentiles for those.
You should expect your child to be on a different percentile for height and for weight. Nature works that way. Someone could be 75th percentile weight and 50th percentile height and they might look slim.
Maybe you were traumatised by maths in childhood. Here's a picture to relax you. What would you say — 90th percentile for cuteness?

BMI in children
For children, statisticians take into account not just height and weight, but also age and sex. You can't show that on a two-dimensional chart, so agencies put up calculators, where you input sex, age, height and weight and out pops a weight which is often labelled 'ideal'.
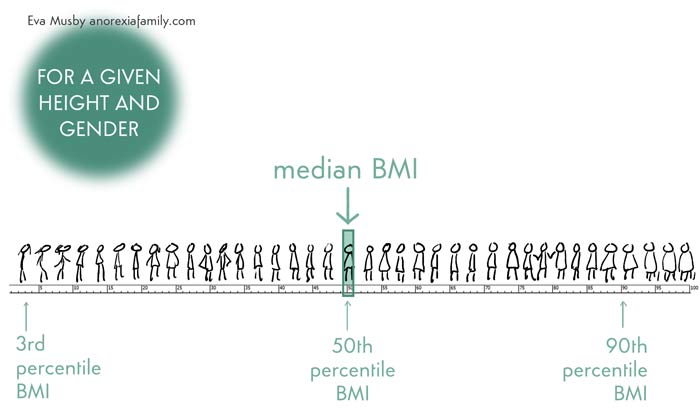
This is the weight that corresponds to the median — or middle – or 50th percentile – BMI:
As you can imagine, given the wide range of what's normal in the population, it's worrying when anyone is told they can or should be right in the middle.
Some calculators do a bit better and present you with a range, like this:

To not add to the harm, I obscured the weight figure.
This calculator's green zone (labelled 'healthy weight') is very wide. That's because when you take a whole lot of kids the same sex, age and height, you get a wide range of weights. Because most kids are healthy, agencies have labelled this wide middle zone as 'healthy'.
But we can't tell if an individual is healthy just because they're in that weight zone.
As an illustration, consider this frustrating story I heard from a mother the other day. Her daughter was 'skin and bones' after months of anorexia-driven restriction. The clinicians warned that she should regain weight urgently, or she would have to be hospitalised. Once home, the girl typed in her data using the health service calculator above, and announced that no way was she going to gain weight. You've guessed it: she was still within the calculators' green 'healthy' range.
Likewise there are kids calculated as 'overweight' who are a picture of health and have a very average-looking body shape. (I hate talking about 'looks' and fatness, but I am guessing many readers need that clarity.)
These errors happen a lot. Healthy kids calculated to be 'overweight' and malnourished kids calculated to have a 'healthy weight'. BMI is such a blunt instrument that sometimes it can't even cut through butter.
Such tools should only be of interest to researchers and statisticians. What calculators should really be saying is this:
"We measured loads of girls [this] age and [this] height, and found a big range of weights. We're showing you the middle BMI, which corresponds to [this] weight. We labelled the extreme ends of the BMI range 'underweight' and 'overweight', and everything in between we labelled 'healthy', shown in green. We deal with big numbers so we don't know who would actually be healthy or unhealthy in any of those zones. No doubt there were some tragically unhealthy, underweight kids in the green zone, and no doubt there were healthy and normal-looking kids in the orange zone."
I hope the shoe analogy helps you to understand the error for yourselves, and it might — just might — help explain it to your child. As eating disorders come with distorted thinking, your child will probably not believe you, which is why the family-based approach is a blessing because it doesn't wait for our children's buy-in.
Let's move on. Because children's BMI depends so much on sex, and age, researchers find it convenient to use 'weight-for-height' instead. Again, this is being misused as a clinical tool, when it should only be used as a research/statistical tool.
What's percent weight-for-height (WFH)?
Weight-for-height is a measure of a child's BMI (body mass index) relative to the middle BMI of a whole lot of kids the same sex and age.
If a child's BMI is bang in the middle of the population's ('median', or on the 50th percentile) then their weight-for-height is 100 percent. In a big population, half the kids have a higher BMI, and half have a lower BMI.
(In the image below, I deliberately didn't draw the girls consistently from thin to fat, because away from the extremes, BMI is not a good indicator of body shape).

If your child weighs 80 percent of this target weight, their BMI is also 80 percent of the median BMI, and you will be told your child is at 80 percent weight-for-height.
When a clinician tracks progress at each visit by logging your child's 'weight-for-height', it's probably because they're using 100 per cent (or less) as a target. (I call this a 'one-size-fits-all method and say more about it here.) Otherwise they would just track your child's weight to make sure that refeeding is working.
Does percentile weight have to match percentile height?
No.
First, because your child's weight has to be whatever turns out to correspond to good physical and mental health. This should not be about numbers.
And second, it is not correct that 100 percent weight-for-height means that someone's weight and height percentiles are identical. It means the person has an average (median, or 50th percentile) BMI, for their sex and age.
I looked up some charts to illustrate this point with two girls enjoying great health:
- Tall Theresa, age 16, is much taller than average, on the 99th percentile for height. Her BMI is average — she's at 100 percent weight-for-height. She is not on the 99th percentile for weight, but on the 60th.
- Petite Patricia, age 16, is much shorter than average, on the 3rd percentile for height. Her BMI is average — she's at 100 percent weight-for-height. She is not on the 3rd percentile for weight, but on the 12th. If Patricia got ill and needed weight-restored, it would be woefully insufficient to stop weight-regain at the 3rd percentile (it would short-change her body by 4 kg).
What is BMI z score?
Some clinicians may calculate your child's BMI z score. So what is it?
It measures the degree of deviation from the median. Just how much of an outlier your child is, in terms of their BMI.
Consider the middle point in the range of BMIs in kids the same sex and age as your child's. (As we've seen, that's also called median BMI and it corresponds to '100 percent weight for height'). The z score is a measure of how far your child's BMI is from that middle point.
More precisely, for those of you who remember statistics from school, the BMI z score is a measure of how many standard deviations a child's BMI is above or below the average BMI for their age and gender. It's used for people age 2 to 20.
It looks to me like the BMI z score might be a popular proxy, among clinicians, for adiposity. You will know how much attention is being paid to 'obesity' in children: recording that a kid's BMI z score is high is a handy shortcut.
And with anorexia, alarm is raised with a very low z score (a big negative number — so for instance a z score of -3 corresponds to a lower BMI than a z score of -1).
Just like % median BMI and % weight-for-height, in isolation, the BMI z score is a very poor measure of risk: a very low score should of course raise the alarm, but a moderate score might hide an alarming amount or speed of weight loss (see my page on weight suppression and my page on atypical anorexia nervosa.)
In short
BMI is a statistical measure of height and weight, and is not an indicator of any individual person's health (or looks).
The same for weight-for-height, which compares your child's BMI with that of other children of the same age and sex.
Where to next?
To understand quite how unreliable BMI is as a proxy for health, I highly recommend Dr Fiona Willer's podcast 'Unpacking weight science' Episode 3 'How we got here: BMI meets death'
More from me on weight restoration
* My main page on weight: Weight-restoration: why and how much weight gain? *
* Experts say, "Recovery weight must be individualized" *
* Is your child's target weight a gift to the eating disorder? *
* Weight gain in growth spurts *
* Weight centile growth charts: why they can’t predict your child’s recovery weight *
* My YouTube: Growth charts and goal weights made simple *
* My YouTube: What is a BMI or '% Weight-for-Height' target, and how wrong it could be *
* Atypical anorexia diagnosis? Handle with care! *
* How much weight did your child lose? Weight suppression is critical in eating disorder diagnosis and treatment *
And there's more:
* More on weight and feeding in Chapter 6 of my book and in my Bitesize audio collection *


#Links: weight-target
Last updated on:
Comments
This is the first time I have seen Arfid mentioned. This helps greatly but even with a diagnosis these percentiles and calculations are still being used sadly. Our son has Arfid and is on the percentiles but deficient. Trying to get help is like banging your head against a brick wall. Thankyou
Dear GA, yes, this topic is one that causes massive frustration among parents… and among clinicians who have tried and failed to get their colleagues to change. Even the quotes I provide from the experts who tend to train these clinicians, too often turn out to be of no avail. Then the only step I know has worked for some is to 'agree to disagree' and for parents to secure an agreement to introduce some changes, then review.
Sending my love and best wishes, Eva
My child has recently been assessed and told she doesn't have an eating disorder because she isn't trying to lose weight or having rules around food or body shape. Although they said she is using not eating as a coping strategy. She had lost weight as she is severely restricting food and fluid and is now struggling physically with attending school due to how she is physically. She says she can't eat because of feelings of guilt and she is distressed when she does eat. I had anorexia and she is exhibiting all the symptoms around food taking ages over trying to eat breaking food up, distress, unable to make decisions around food etc..
Historically she has been on the 50th centile and is now on the 5th. I am concerned because this isn't being called an eating disorder there is no encouragement to weight restore, and through my support we have stabilised her low weight. It is very concerning.Hello Riddle, yes, I can well imagine how concerning it is to you. What you describe sounds to me like one of the eating disorders under DSM-5. If it's not anorexia it might come under ARFID or OSFED. (I describe these classifications on https://anorexiafamily.com/classification-eating-disorders) Either way it seems to me essential she gets specialist treatment and you get the help too. I am guessing you are in the UK and so the NHS has a duty to give her access to this. If not, definitely ask for a second opinion e.g. from the Maudsley: my understanding is that it's a national centre of expertise that any trust has access to.
Another thought is that sometimes youngsters appear to not have concerns around weight or shape, but that's only while they can eat very little. For some, when refeeding starts with full meals, then distress around weight gain may become apparent.
I hope you get the help you need. Love, Eva
My child has emetophobia (a fear of being sick) and is very anxious about food. Although he will eat most things willingly, the amount can cause issues (I feel too full…will this make me sick?) I've recently weighed him as it was becoming apparent that the amount he was eating was nowhere near enough for a growing teenager. He's on the 1st percentile which is classed as underweight on the charts. His counsellor has said that this is nothing to worry about, but it's clearly affecting him as he has no energy, won't exercise, and always feels tired. I want him to gain weight but don't want to trigger any additional anxiety over food. Is this weight really 'nothing to worry about'?
Hello there, your child's health is at risk. He has a psychological illness called ARFID. Please do speak to a doctor urgently as he certainly needs help to overcome his mental illness. Its best the intervene with the issue early on to prevent it being a life long problem with many health consequences. ARFID is as serious as anorexia nervosa, if not more.
Ruby, I am so glad you wrote this. Somehow I had missed EmetoMum's message.
For those needing more info on ARFID, see the books and links I list on https://anorexiafamily.com/classification-eating-disorders#ARFID
Eva
LEAVE A COMMENT (parents, use a nickname)